What is a Hernia?
| A hernia (rupture) is usually noticed as
a lump, commonly in the groin or the umbilical region. |
 |
It appears when a portion of the tissue
which lines the abdominal cavity (peritoneum)
breaks through a weakened area of the
abdominal wall.
This can give rise to discomfort as the
hernia enlarges and can sometimes be
dangerous if a piece of intestine
becomes trapped ('strangulated') inside.
There is almost no limit to how BIG a
hernia could get if left untreated! |
The Anatomy of HERNIA
The most common
location for hernia is the abdomen. The abdominal wall - a sheet of tough
muscle and tendon that runs down from the ribs to the legs  at
the groins - acts as 'nature's corset'. Its function, amongst other things,
is to hold in the abdominal contents, principally the intestines. at
the groins - acts as 'nature's corset'. Its function, amongst other things,
is to hold in the abdominal contents, principally the intestines.
If a weakness should open up in
that wall, and it does not really matter how or why it happened (more on
this later), then the 'CORSET EFFECT' is lost and what pushes against
it from the inside (the intestines) simply pushes through the 'window'.
The ensuing bulge, which is often quite visible against the skin, is the
hernia.
These 'windows of weakness' commonly
occur where there are natural weaknesses in our abdominal wall - such as
where the 'plumbing' goes through it. Examples of these are the canals
(inguinal and femoral) which allow passage of vessels down to the scrotum
and the legs, respectively. The umbilical area (navel) is another area
of natural weakness frequently prone to hernia. Another area of potential
weakness can be the site(s) of any previous abdominal surgery. |
What to do about a HERNIA
The ONLY way to stop a hernia
getting worse is to repair the defect surgically. There are, however, several
ways of doing this and the results vary widely. What follows explains most
of them and describes various aspects related to the different types of
hernia.
Hernia Terminology
GROIN
HERNIAS: |
-
Inguinal Hernia
-
Femoral Hernia
-
Scrotal Hernia
|
Any of these can be
Primary ('first time')
or
Recurrrent hernias |
OTHER
HERNIAS: |
-
Ventral Hernia
-
Umbilical Hernia
-
Ventral / Epigastric Hernia
-
Incisional Hernia
-
Spigelian Hernia
-
Recurrent Hernia
-
Recurrent Incisional Hernia
-
Bilateral (or 'double') Hernia
-
Stoma Hernia
-
Hiatus Hernia
|
Although all carry the word
'Hernia' the following text relates to all but the Hiatus hernia.
|
Who can get a Hernia?
Anybody, of either sex and at any age.
How do Hernias happen?
The wall of the abdomen, comprising muscle and tendon,
performs several functions, one of which is to provide strong support to
the internal organs which are exerting significant outward pressure. The
opening of a gap in the tissue can occur of its own accord at a point of
natural weakness, or by over-stretching a part of the tissue. Overexertion
can cause it, but so could a simple cough or sneeze.
The occurrence of the gap in the abdominal
wall is not normally, of itself, a problem. The problems result from
the ensuing bulge of intestine through the gap. The effects felt by
the patient can range from being perfectly painless, through discomfort,
to being very painful indeed.
Almost every movement we make puts additional
pressure on the internal tissues which, in turn, push out through the opening
a little more each time. This also enlarges the opening itself. If unchecked,
this process can continue even to the extent of allowing much of the intestine
to hang down through the hernia.
Sport,
Groin Pain and Hernia
Groin pain is a frequent
disability commonly seen in golfers and other sports players
and athletes.  In
certain muscle strains and tears, the sequence is acute groin pain which,
at first, can be completely crippling, then gradually subsiding with chronic,
repetitive, sharp pain and aching groin - more marked with certain movements. In
certain muscle strains and tears, the sequence is acute groin pain which,
at first, can be completely crippling, then gradually subsiding with chronic,
repetitive, sharp pain and aching groin - more marked with certain movements.
Some patients have an associated lump, which commonly
indicates an inguinal hernia.
The first treatment, frequently given to professional
sportsmen, is intensive physiotherapy, ultrasound, injections and graduated
exercise. This is often successful in healing muscle strains.
Where a lump is present, however, early surgery
is necessary. Where no lump is apparent and where physiotherapy (as
above) fails to correct the problem, it is possible that the groin-area
muscles have torn. This tear must be repaired, a procedure which gives
good results.
In any case, it is essential
to diagnose correctly whether the problem is a 'Groin
Strain', a Torn
Muscle or a HERNIA.
One must avoid giving the treatment for one when the condition is another!
Sometimes, many find it difficult to distinguish
which condition exists.
BY NO MEANS is surgery required in all
cases, especially where there is no swelling. True experts in hernia would
not rush into surgery, so it is essential to consult specialists who regularly
see all these kinds of cases.
|
Where required, these various injuries are treated
surgically as day cases under local anaesthesia
and allow a return to full - even vigorous - training, usually within 2
to 3 weeks. |
Can Hernias get better?
The opening of a hernia cannot heal
itself, neither can any medicine be used to cure the condition.
The long term course, therefore, is for a hernia
to become steadily worse as time goes on,
sometimes slowly and sometimes quickly.
The only remedy for the condition is to repair the
hernia surgically, but that no longer means you have
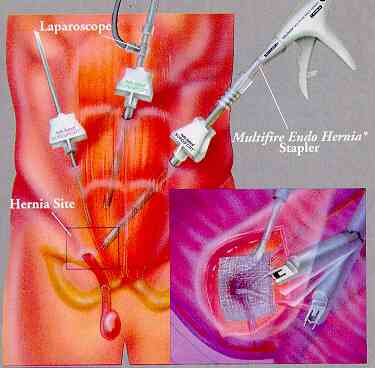
to be an invalid afterwards. Below is one of the newer surgery procedures for a inguinal hernia.
LAPAROSCOPIC INGUINAL
HERNIA REPAIR
The information is provided by
THE BRITISH HERNIA CENTRE
London, England
|

